Patient no-shows cost healthcare $150B annually. Learn how predictive scheduling, automated reminders, and centralized models reduce no-shows by 25-40%.
by
VitalCX Healthcare Operations Team

February 17, 2026


9 minutes
Patient no-shows cost the U.S. healthcare system an estimated $150 billion annually, with average no-show rates ranging from 15% to 30% across ambulatory care settings. The problem is not patient irresponsibility — it is a systems failure rooted in scheduling friction, access barriers, and inadequate patient communication. Healthcare organizations that deploy predictive scheduling, automated reminders, and centralized access models consistently reduce no-show rates by 25–40% while improving provider utilization and downstream revenue.

The financial impact of patient no-shows extends far beyond a single missed appointment. According to data from the Healthcare Financial Management Association (HFMA), the average cost of a single no-show ranges from $200 to $400 depending on specialty, factoring in lost revenue, idle staff time, and unused clinical resources. Across the U.S. healthcare system, that adds up to approximately $150 billion per year.
For a mid-sized health system with 500 providers, a 20% no-show rate can translate to $10–15 million in annual lost revenue. That figure doesn't account for the downstream effects: delayed diagnoses, worsened chronic conditions, and increased emergency department utilization that follow when patients miss scheduled care.
The American Medical Association (AMA) reports that primary care practices experience no-show rates between 15% and 23%, while specialty practices — particularly behavioral health, dermatology, and pain management — see rates as high as 30%. Safety-net clinics serving Medicaid populations often exceed 30%.
The math is straightforward: every 1% reduction in no-show rate for a 200-provider organization recovers roughly $500,000–$1 million annually. Scheduling optimization isn't a convenience project. It's a revenue recovery strategy.
The instinct to blame patients for no-shows misses the structural reality. Research published in the Journal of General Internal Medicine and confirmed by multiple NAHAM (National Association of Healthcare Access Management) studies identifies consistent systemic drivers:
Transportation barriers. The American Hospital Association (AHA) reports that 3.6 million Americans miss medical appointments annually due to transportation issues. This disproportionately affects Medicaid, rural, and elderly populations.
Long lead times. Appointments scheduled more than two weeks out have dramatically higher no-show rates. A 2024 study in Health Affairs found that appointments booked 30+ days in advance had no-show rates 2.5x higher than those booked within 7 days.
Scheduling friction. When patients must call during business hours, navigate phone trees, and wait on hold, the scheduling process itself becomes a barrier. Organizations with digital self-scheduling see 15–20% lower no-show rates than those relying solely on phone-based booking (see [Blog 7] on digital front doors).
Lack of reminders. Practices sending no reminders or single reminders see significantly higher no-show rates than those using multi-touch, multi-channel reminder sequences.
Financial concerns. Patients uncertain about out-of-pocket costs or insurance coverage are more likely to avoid appointments altogether. Real-time eligibility verification at scheduling (covered in [Blog 5]) directly addresses this driver.
Appointment complexity. Patients who don't understand why they need a visit — or what to bring, expect, or prepare — are more likely to skip it.
The takeaway: no-show rates are a symptom. The disease is operational friction.
Predictive scheduling uses historical patient data, demographic factors, and appointment characteristics to estimate no-show probability for each scheduled visit. Organizations using predictive models report 25–40% reductions in no-show rates, according to studies published in the Journal of the American Medical Informatics Association (JAMIA).
How it works:
Predictive models pull from multiple data sources:
Machine learning algorithms — typically gradient boosting or logistic regression models — assign a no-show risk score to each appointment. That score drives three operational interventions:
Cleveland Clinic, Geisinger, and Kaiser Permanente have all published results showing 25–35% no-show reductions using predictive scheduling. Smaller health systems using vendor-based predictive tools report similar results in the 20–40% range.
The key insight: predictive scheduling doesn't eliminate no-shows. It converts a random problem into a manageable one by concentrating intervention resources where they matter most.
Automated Reminders — SMS, Voice, App-Based
Automated appointment reminders are the most widely adopted no-show intervention, and the evidence supporting multi-channel, multi-touch sequences is overwhelming.
Effectiveness by channel:
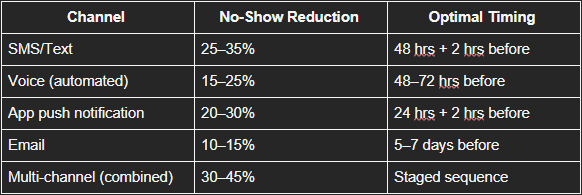
NAHAM's 2025 Patient Access Benchmarking Survey found that organizations using three or more reminder touchpoints across at least two channels achieved the lowest no-show rates in their cohort.
Best practices for reminder programs:
The reminder program is not a standalone solution. It works best when paired with predictive targeting (concentrating extra reminders on high-risk appointments) and self-service rescheduling tools (see [Blog 7]).
Centralized vs. Decentralized Scheduling Models
The scheduling model itself — who schedules, where, and with what tools — has a direct impact on no-show rates, provider utilization, and patient access.
Decentralized scheduling (each department or clinic manages its own scheduling) is the legacy model in most health systems. It creates:
Centralized scheduling consolidates scheduling into a unified access center — either physical or virtual — with standardized protocols, shared visibility into all provider schedules, and coordinated patient communication.
Organizations that have moved to centralized scheduling report:
The centralized model enables the "right patient, right provider, right time" principle. When a scheduler has visibility into the entire network, they can match clinical need to provider availability, account for patient preferences, and optimize geographic convenience — all of which reduce no-shows.
Hybrid models are emerging as the practical middle ground. Clinical teams retain control over complex scheduling decisions (surgical coordination, multi-visit treatment plans), while routine scheduling flows through a centralized access center. This preserves clinical autonomy while capturing the efficiency and consistency benefits of centralization.
CMS's emphasis on timely access in value-based care programs (MIPS, ACO REACH) is accelerating the shift toward centralized models. Organizations that can demonstrate shorter time-to-appointment and lower no-show rates gain advantages in quality scoring and shared savings calculations (see [Blog 18]).








