Hospital revenue cycle management in 2026: denial rates hit 10-15%, rework costs $25-$118 per claim. Learn the 7 RCM stages and AI strategies.
by
VitalCX Healthcare Operations Team

April 5, 2026


7 minutes
Revenue cycle management (RCM) is the end-to-end financial process that healthcare organizations use to track patient care episodes from registration and appointment scheduling through final payment of a balance. In 2026, RCM has become the single most important operational discipline for hospital survival — not because clinical care has gotten worse, but because the financial complexity surrounding that care has made it nearly impossible to get paid correctly the first time.
Hospitals don't fail because they deliver bad care. They fail because they can't collect for the care they deliver.
Revenue cycle management encompasses every administrative and clinical function that contributes to the capture, management, and collection of patient service revenue. According to the Healthcare Financial Management Association (HFMA), the revenue cycle includes all activities from the moment a patient schedules an appointment to the moment the provider receives final payment.
In 2026, three forces have made RCM existentially important:
1. Payer complexity has exploded. The average hospital now contracts with 15–20 commercial payers, each with different authorization requirements, timely filing limits, and reimbursement methodologies. Medicare Advantage enrollment has surpassed 54% of all Medicare beneficiaries (CMS, 2025), bringing commercial-style utilization management into what was once the most straightforward payer relationship in healthcare.
2. Operating margins are razor-thin. The American Hospital Association (AHA) reported that more than half of U.S. hospitals operated at a negative margin in 2024. Labor costs have risen 20%+ since 2020 while reimbursement rates have remained flat or declined in real terms. There is no room for revenue leakage.
3. Regulatory requirements keep expanding. The No Surprises Act, CMS price transparency rules, and state-level balance billing protections have added compliance layers that directly impact how charges are captured, billed, and collected. Non-compliance carries financial penalties and reputational risk.
The result: RCM is no longer the billing department's problem. It is an enterprise-wide operational discipline that touches registration, clinical documentation, coding, charge capture, claims submission, payment posting, denial management, and patient collections.

Denial rates across U.S. hospitals currently range from 10% to 15% of all submitted claims, according to data from the Medical Group Management Association (MGMA) and HFMA. Some specialties — particularly those requiring prior authorization, such as cardiology, orthopedics, and oncology — see denial rates exceeding 20%.
Here's what makes these numbers dangerous:
The math is brutal. A 300-bed community hospital generating $500M in net patient revenue with a 12% denial rate faces $60M in initially denied claims. If 65% are never appealed, that's $39M left on the table before a single dollar of rework cost is calculated.
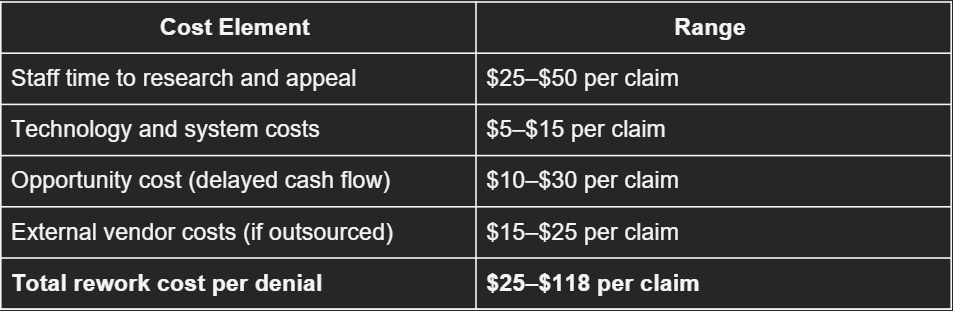
The cost of a denied claim goes far beyond the face value of the charge. HFMA estimates that reworking a single denied claim costs between $25 and $118, depending on the complexity of the denial and the payer involved.
Here's the cost breakdown:
For a hospital processing 200,000 claims per year with a 12% denial rate, that's 24,000 denied claims. At an average rework cost of $50 per claim, the hospital spends $1.2M annually just on denial rework — and that's before accounting for the claims that are never recovered.
The Advisory Board estimates that denial-related revenue leakage — the combination of rework costs and unrecovered write-offs — costs the average health system between $3.3M and $4.9M per year.
Every revenue cycle follows a sequential process. Failure at any stage compounds downstream. The seven stages are:
Stage 1: Pre-Registration and Scheduling. Capturing accurate patient demographics, insurance information, and verifying eligibility before the patient arrives. Errors here are the root cause of 25–30% of all downstream denials (NAHAM). → See Blog 5: Patient Access in Healthcare
Stage 2: Registration and Check-In. Confirming and updating information at the point of service. This includes collecting copays, verifying identity, and executing Advance Beneficiary Notices (ABNs) for Medicare patients when coverage is uncertain.
Stage 3: Charge Capture. Documenting all billable services, procedures, and supplies during the patient encounter. Missed charges cost mid-size health systems $10M+ annually. → See Blog 3: Charge Capture in Healthcare
Stage 4: Coding. Translating clinical documentation into ICD-10, CPT, and HCPCS codes. Coding accuracy directly determines reimbursement accuracy. The American Medical Association (AMA) maintains CPT code sets; CMS maintains ICD-10-CM/PCS.
Stage 5: Claims Submission. Generating and transmitting clean claims to payers. A "clean claim" — one that passes all edits and requires no additional information — should be submitted within 24–48 hours of the encounter for optimal cash flow.
Stage 6: Payment Posting and Reconciliation. Receiving and posting payer remittances, identifying underpayments, and reconciling expected vs. actual reimbursement against contracted rates.
Stage 7: Denial Management and Collections. Working denied claims, filing appeals, and managing patient balances. This stage is where most revenue cycle teams spend disproportionate time and resources. → See Blog 2: Healthcare Claim Denial Management
The most effective revenue cycle operations focus resources on stages 1–5 (prevention) rather than stages 6–7 (recovery). Prevention is always cheaper than rework.

The health systems that are outperforming on RCM metrics in 2026 share several common strategies:
Centralized revenue cycle operations. Rather than allowing each facility or department to manage its own billing, leading systems have consolidated RCM into centralized shared services. This enables standardized processes, better analytics, and more efficient staffing. HFMA reports that centralized RCM operations achieve 5–10% lower cost-to-collect ratios than decentralized models.
Front-end investment. The highest-performing organizations invest disproportionately in patient access — real-time eligibility verification, automated prior authorization, and digital patient intake. Every dollar spent on front-end accuracy saves $5–$10 on back-end rework.
Denial prevention over denial management. Instead of building larger appeal teams, leading systems analyze denial root causes and implement upstream corrections. A robust denial prevention program targets the top 5 denial reason codes (which typically account for 60–70% of all denials) with specific process interventions.
Contract management discipline. Underpayments from commercial payers cost hospitals 1–3% of net revenue annually. Leading systems use automated contract management tools to compare every remittance against contracted rates and flag variances in real time.
Workforce model redesign. With revenue cycle labor costs rising and experienced coders and billers in short supply, health systems are deploying a hybrid model: automation for high-volume, rules-based tasks (eligibility checks, claim scrubbing, payment posting) and skilled staff for complex work (clinical appeals, underpayment negotiations, coding audits).
1. Predictive denial prevention. Machine learning models trained on historical denial data can flag claims likely to be denied before submission. Early-adopter health systems report 20–30% reductions in initial denial rates using predictive analytics to route high-risk claims for pre-submission review.
2. Automated coding assistance. Natural language processing (NLP) tools can suggest ICD-10 and CPT codes based on clinical documentation, reducing coding lag time and improving accuracy. The AMA and AHIMA have both issued guidance on responsible use of AI in coding workflows.
3. Intelligent claims follow-up. AI-powered worklist prioritization helps denial management teams focus on the highest-value, highest-probability-of-recovery claims first, rather than working denials in FIFO order.
What AI does not do — and likely will not do in the near term — is replace the need for process design, payer relationship management, or clinical documentation improvement. AI is an accelerant, not a substitute for operational discipline.
The health systems getting the most from AI in RCM are the ones that fixed their processes first and then layered technology on top. The ones expecting AI to fix broken workflows are spending money without moving metrics.








